Pressure ulcer management with Flaminal®
Tissue damage from prolonged pressure — clinical approach to dressing selection, staging, and exudate control.
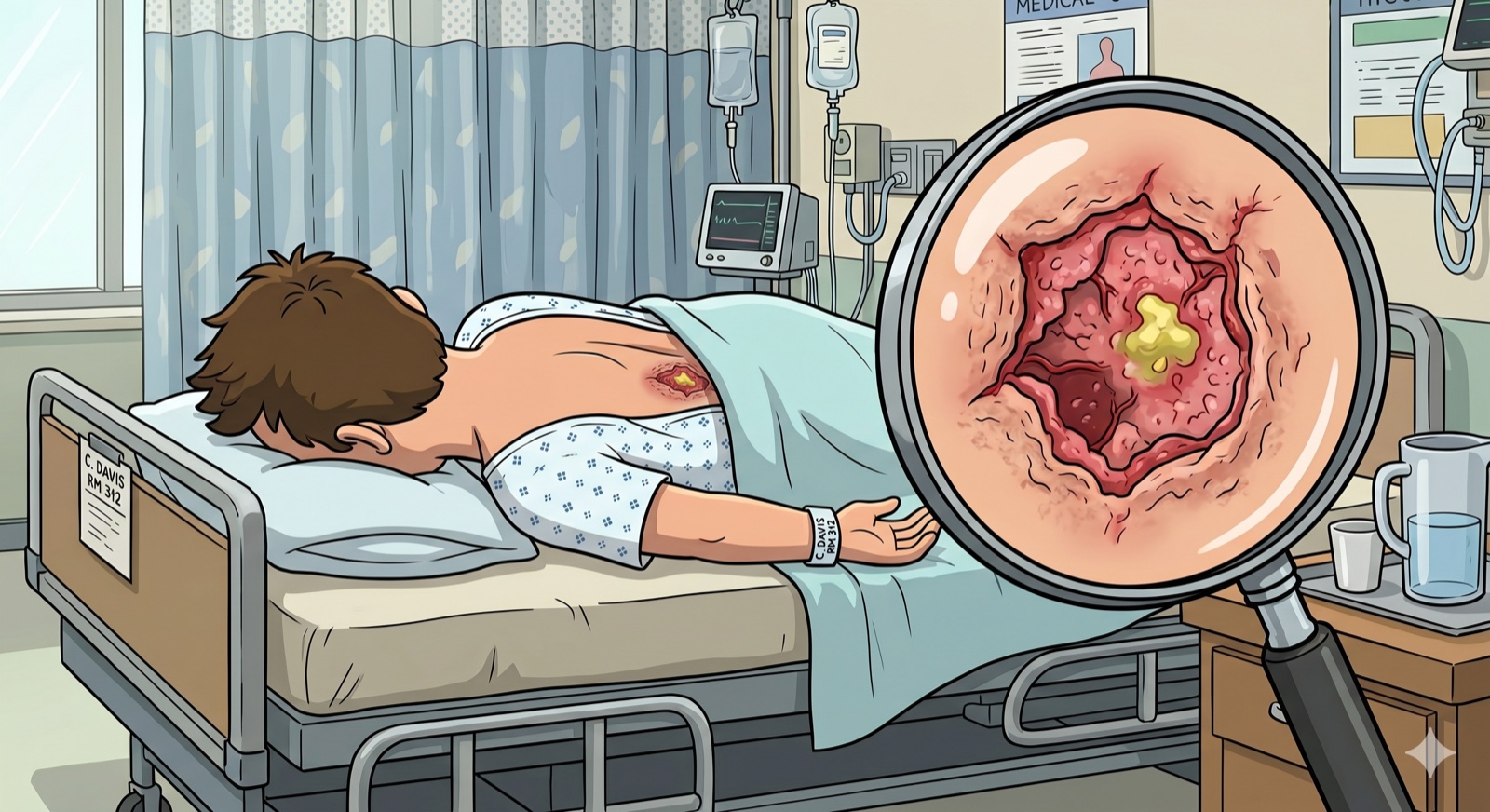
What is a pressure ulcer
A pressure ulcer is localised damage to the skin and underlying tissue caused by sustained pressure or pressure combined with shear. It develops most often over bony prominences (sacrum, heels, ischial tuberosities, scapulae) in immobilised patients. The international NPUAP/EPUAP/PPPIA classification (2019) defines four stages plus two additional categories.
What it looks like in practice
2 real-world cases from clinics using Flaminal® — before/after photos, treatment protocol, and healing timelines.
Real clinical cases from the practice of partner clinics using Flaminal® in Uzbekistan. Patient personal data is not published.
NPUAP/EPUAP stages
Stage determines dressing choice and care plan
Stage I
Non-blanching erythema on intact skin. Colour, temperature, firmness or sensation changes in the at-risk area.
Stage II
Partial-thickness skin loss (epidermis ± part of dermis). Shallow open ulcer with a red-pink bed, no slough, or an intact/ruptured blister.
Stage III
Full-thickness skin loss. Subcutaneous fat may be visible but bone, tendon and muscle are not. Slough, tunneling or undermining may be present.
Stage IV
Full-thickness tissue loss with exposed bone, tendon or muscle. Slough and undermining are often present. High osteomyelitis risk.
Unstageable / DTI
Unstageable — depth is obscured by slough or eschar. Deep tissue injury (DTI) — localised purple/maroon area of intact or non-intact skin signalling deep injury; outcome unpredictable.
Treatment principles
NPUAP/EPUAP/PPPIA 2019 — four pillars
Pressure offloading
Reposition every 2 hours, use pressure-redistribution mattresses and cushions, and dedicated heel offloaders. Without offloading no dressing works.
Cleansing and debridement
Remove necrotic tissue and slough per the TIME framework. Enzymatic, autolytic or surgical methods as indicated.
Microbial load control
Topical antimicrobial therapy for critical colonisation and biofilm. Systemic antibiotics only for systemic infection guided by culture.
Moisture balance
A moist environment accelerates epithelialisation. Match the dressing to exudate volume: gels and hydrocolloids for dry wounds, alginates and foams for exuding wounds.
Where Flaminal® fits in this scenario
Flaminal®'s enzymatic gel acts across stages II–IV. Glucose oxidase and lactoperoxidase gently break down necrotic tissue and sustain antimicrobial action without antibiotics. The alginate matrix absorbs exudate and maintains a moist environment. The gel does not adhere to new granulation tissue — important for patients with long treatment courses and frequent dressing changes.
Flaminal Hydro
Low exudate.
Flaminal Forte
Heavy exudate.
Supporting studies
Wound-bed preparation with an enzyme alginogel in the treatment of pressure ulcers
Bernaerts K. et al. · Journal of Wound Care · 2012
On requestClinical review: Flaminal® in complex pressure ulcers
White R., Cowan T. · Wounds UK · 2014
On requestInternational Clinical Practice Guideline for Prevention and Treatment of Pressure Ulcers
NPUAP / EPUAP / PPPIA · Clinical Guideline, 3rd ed. · 2019
On request
Further reading
More on the manufacturer's site
Flen Health maintains a detailed topic page with clinical cases. Opens in a new tab.